
When the Pain Refuses to Leave: The Hidden Role of Microbial Colonies in Unresolved Injury
Why some injuries keep hurting long after they should have healed — and what the science of biofilms and terrain coherence tells us about why.
DISCLAIMER: The content of this post is educational and informational only. PHOENIX SANCTUM™ does not diagnose, treat, cure, or prevent any disease or medical condition. Nothing in this post constitutes medical advice. Please consult your healthcare practitioner for any medical concerns.
You Did Everything Right. The Pain Stayed Anyway.
You rested. You saw the physio. You stretched, iced, compressed, elevated. Maybe you had an ultrasound, a cortisone injection, or a course of anti-inflammatories. And yet, weeks turned to months. The swelling ebbed. The bruising faded. But the pain — that dull, insistent ache in the knee, the ankle, the shoulder, the spine — never quite left.
This is one of the most common and most misunderstood experiences in musculoskeletal health. A person sustains an injury. By every conventional measure, it should have resolved. Imaging looks clear. Bloodwork appears normal. And still, the area hurts — sometimes for years.
What most people are never told is that there may be a reason their body hasn't finished the job — and it has nothing to do with their willpower, their pain threshold, or the quality of their physiotherapy. It may have everything to do with something far smaller, and far more tenacious: microbial life, quietly colonising the site of an old wound.
The Biology of Persistence: What Biofilms Actually Are
When bacteria enter a wound — through a tear, a trauma, a surgical incision, or even the micro-damage that accompanies a significant strain — the first thing most people imagine is an acute infection: redness, warmth, swelling, fever. That is one scenario. But bacteria are opportunists with long memories. They are also engineers.
Under the right conditions, bacteria can organise themselves into what scientists call biofilms — structured communities of microorganisms encased in a self-produced matrix of polysaccharides, proteins, and extracellular DNA. This matrix acts as both a physical shield and a biochemical fortress. Within it, individual bacteria can enter a metabolically dormant state, dramatically reducing their profile to the immune system and rendering them up to a thousand times more resistant to antibiotic therapy than their free-floating counterparts.
The science here is not fringe. A landmark 1999 paper in Science by Costerton et al. established that biofilm-forming bacteria are implicated in the vast majority of persistent human infections. Research published in Nature Reviews Microbiology by Hall-Stoodley, Costerton and Stoodley confirmed that biofilms are found not only on medical devices and wound surfaces, but in musculoskeletal tissues — including bone — where they can persist in a chronically quiescent state, periodically releasing free-roaming bacteria that trigger flares of symptoms before retreating back into the protection of the matrix. [1, 2]
Research on orthopaedic biofilm infections — reviewed extensively in Frontiers in Microbiology — has demonstrated that conventional microbiological culture techniques detect biofilm-associated organisms only around 30% of the time, compared with rates of 80–90% using histology and microscopy. [3] This is not a minor discrepancy. It means the standard tests used to rule out infection at an injury site will miss the vast majority of established biofilms. An injury is declared 'not infected', and the patient continues to live with unexplained, unresolved pain.
Bone, Ligament, and Tendon: Not Just Structural — Microbially Vulnerable
It is tempting to think of bones and ligaments as sterile, well-defended structures. In reality, they are among the most immunologically challenging tissues in the body to defend once a pathogen gains a foothold.
Research from the University of Rochester's Center for Musculoskeletal Research has shown that certain bacterial strains — most notably Staphylococcus aureus — can physically penetrate the canalicular network of cortical bone, colonising spaces so narrow that immune cells simply cannot follow. Once embedded in these micro-channels, bacteria can persist indefinitely while the surrounding tissue remains in a state of low-grade, chronic inflammatory activation. [4]
For ligament and tendon tissue, the picture is similarly complex. A systematic review published in BMC Musculoskeletal Disorders found persistent inflammatory markers in tendinopathic tissues years after the initial injury — not because the tendon had been further damaged, but because the immune response had never fully resolved. The identified cell profile was consistent with a chronic persistent stimulus, not with passive degeneration. [5]
This is a distinction with profound practical implications. Chronic tendinopathy is commonly treated as a structural or biomechanical problem — a matter of collagen disorganisation and poor load management. That framing is not wrong, but it may be radically incomplete when a microbial component is sustaining the inflammatory environment and actively preventing tissue reorganisation.
Why Physiotherapy Alone May Not Be Enough
Physiotherapy is one of the most evidence-based interventions available for musculoskeletal injury. Loading tendons progressively, improving local circulation, restoring neuromuscular coordination — these are all genuinely effective strategies for structural rehabilitation. But they are mechanical interventions applied to a biological environment. If that environment is compromised by persistent microbial activity, the structural work may be perpetually undermined.
Think of it this way: you can strengthen the walls of a building all you like, but if the ground beneath it is unstable, the building will keep settling. In musculoskeletal terms, the 'ground' — the informational and biochemical terrain of the injured tissue — needs to be addressed alongside structure.
Research published by Gracey et al. in Nature Reviews Rheumatology established that bacterial infections of barrier surfaces — combined with mechanical stress — can directly hijack the normal healing processes at tendon and ligament attachment sites, driving sustained entheseal inflammation and aberrant tissue repair. [6] In other words, the presence of pathogens at an injury site does not simply add to the problem: it can fundamentally alter the healing trajectory.
This is not a call to abandon physiotherapy. It is a call to consider the full terrain — and to ask whether there is an uninvited occupant in the tissue that no amount of therapeutic loading can evict.
The Circulation Problem: Why the Body Can't Always Get In
Tendons and ligaments are notoriously poorly vascularised relative to other tissues. This is one reason they heal slowly. But it also means that the immune system's capacity to deliver white blood cells, inflammatory mediators, and healing factors to the site of injury is already limited — even under ideal conditions.
When a traumatic injury further disrupts local microcirculation — through bruising, haematoma formation, scar tissue, or chronic oedema — that limitation becomes more severe. The immune system cannot effectively survey the tissue. It cannot clear debris. It cannot mount a sufficient localised response to bacterial colonists who are already sheltering behind a biofilm matrix.
This creates a self-reinforcing pattern: poor circulation allows pathogens to entrench; entrenched pathogens perpetuate inflammation; chronic inflammation contributes to further circulatory compromise; reduced circulation deepens the immune access problem. The body is not failing. It is doing its best under conditions it was not designed to overcome without support.
Supporting the resolution of this pattern requires more than structural intervention. It requires addressing circulation, terrain coherence, informational signalling, and — where pathogenic colonisation is suspected — targeting the organisms that have set up residence in tissues the immune system cannot easily reach.
Frequency, Electromagnetic Fields, and the Science of Disruption
This is where the conversation moves into territory that is both genuinely scientific and frequently misrepresented. Let us be clear about what the research actually shows.
A peer-reviewed study published in Applied Sciences in 2021 demonstrated that specific resonant electromagnetic fields were capable of disrupting biofilm formation in Pseudomonas aeruginosa — a major pathogen in respiratory and wound infections — without affecting planktonic (free-floating) bacterial growth. The research established that weak resonant magnetic fields can interfere selectively with biofilm architecture, and proposed these as a viable non-chemical approach to combating antimicrobial resistance. [7]
A separate study in Scientific Reports (2025) demonstrated frequency-dependent electromagnetic effects on bacterial viability and antibiotic sensitivity. At specific frequencies, previously resistant strains of E. coli and S. aureus became susceptible to antimicrobial agents — not through any chemical mechanism, but through electromagnetic modulation of bacterial behaviour. [8]
The 'bioelectric effect' — the phenomenon by which weak electric currents synergise with antimicrobial agents to dramatically increase pathogen clearance — has been replicated across multiple biofilm systems. A study in Antimicrobial Agents and Chemotherapy demonstrated that radio frequency electric currents could vibrate the polar structures of the biofilm matrix, weakening its integrity and increasing exchange between embedded bacteria and the surrounding environment — effectively opening the fortress to immune access. [9]
None of this proves that any particular frequency device definitively eliminates pathogens in injured human tissue. The research landscape is evolving. But it does establish, beyond reasonable doubt, that electromagnetic and frequency-based interventions have measurable, selective effects on microbial biofilms — and that these effects are real, documented, and increasingly being taken seriously by mainstream microbiology research.
The Role of PEMF, Cold Laser, and TENS in Supporting Healing Terrain

Beyond their potential direct effects on pathogens, technologies such as PEMF, cold laser (low-level laser therapy / LLLT), and electrical stimulation have well-documented roles in restoring the circulatory and cellular conditions that allow natural healing to proceed.
PEMF (pulsed electromagnetic field therapy) has been shown in randomised controlled trial research — including a 2022 study published in BMC Geriatrics — to significantly outperform laser therapy in reducing pain at rest and improving functional outcomes in knee joint conditions. The proposed mechanisms include stimulation of adenosine receptor expression in chondrocytes and synoviocytes, modulation of inflammatory signalling, and improvements in local circulation that enable better nutrient and immune cell delivery to compromised tissue. [10]
Cold laser therapy (LLLT) stimulates cellular ATP production, increases local blood supply, accelerates collagen alignment in healing connective tissue, and has demonstrated pain reduction in chronic joint disorders including tendinitis, fibromyalgia, and myofascial pain. [11] Research suggests that photobiomodulation — the mechanism by which laser light interacts with cell mitochondria — can reduce oxidative stress at the injury site and support the restoration of normal cellular energetics in compromised tissue.
TENS (transcutaneous electrical nerve stimulation), particularly when applied with purpose-selected frequencies via silver conductive wearables in direct contact with the area of interest, adds a further layer: direct electrical stimulation of the local environment that may support tissue conductivity, reduce inflammatory mediator accumulation, and — when combined with frequency-specific programmes — provide a vehicle for resonance-based informational input at the site of concern.
Individually, these technologies support terrain. Together, applied in a structured, sequenced manner with specific intentions and target frequencies, they create conditions that are meaningfully different from a passive inflammatory environment in which pathogens can persist unchallenged.
What We Have Observed: Anecdotal Evidence in Practice
The following are practitioner observations from work conducted at PHOENIX SANCTUM™. These are anecdotal accounts — not clinical trials, not controlled experiments. They are shared as observational data in the spirit of transparency and honest record-keeping. Names have been changed.
Ian's Knee
Ian had been carrying pain and bruising in his knee for over a year. It had never fully resolved despite time and conventional support. When a biofeedback scan was run on the knee — capturing the body's electromagnetic response patterns against a reference database — the results flagged numerous pathogenic resonances in the area. We ran a structured frequency session targeting those specific organisms, alongside programmes associated with local trauma repair and tissue support.
The following day, Ian reported a significant and unexpected reduction in both bruising and pain. Not a subtle shift. A marked one. He described it as the most substantial improvement he had experienced in the preceding twelve months. We share this not as proof of mechanism, but as an observation worth recording: that when the biofeedback data suggested a microbial load at the injury site, and when frequencies associated with those organisms were applied alongside healing support programmes, the response was notable.
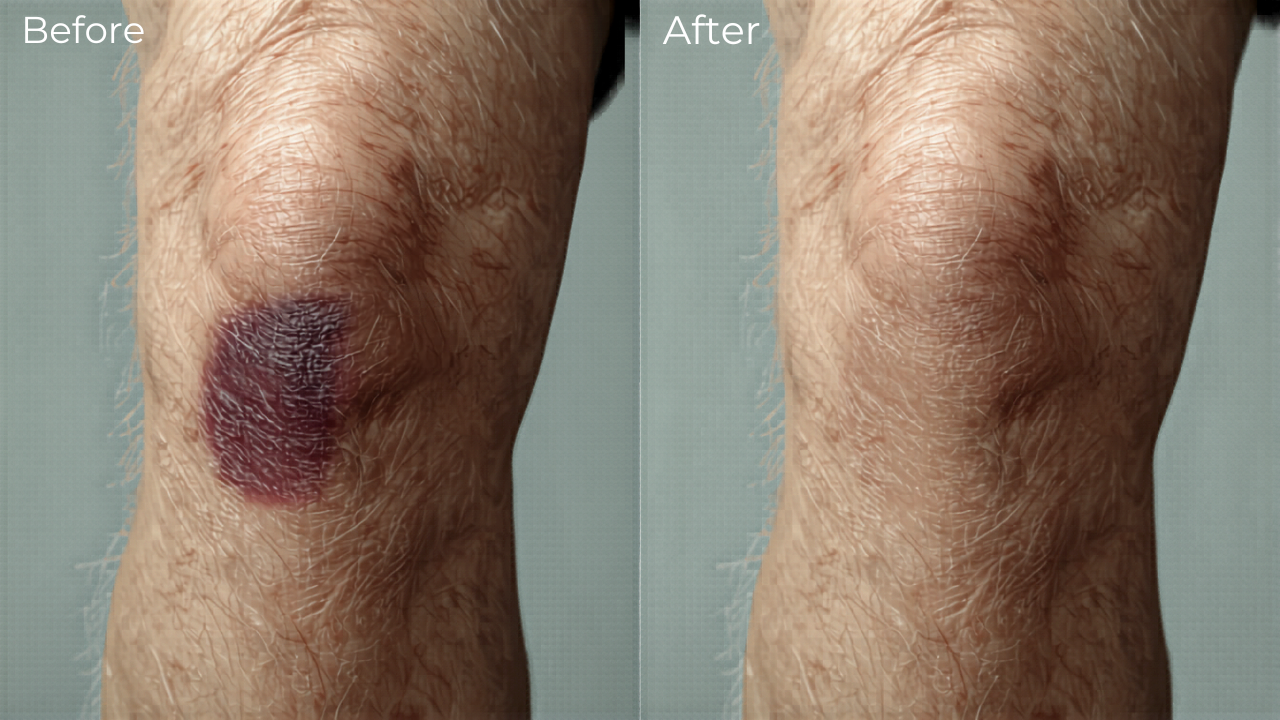
Illustrative example:
Old traumas may benefit from targeted TENS frequency support
Keith's Ankle
Keith twisted his ankle and came in shortly after the injury. By all expectations — based on the mechanics of the twist and the initial presentation — significant swelling and pain were to be expected over the following day. We ran a fifteen-minute session using TENS silver bands applied directly to the ankle, with frequency programmes targeting both pathogenic resonances associated with traumatic injury sites and localised tissue repair and inflammation support.
The next morning, Keith woke up expecting the anticipated pain and limitation. He found neither. The swelling had not materialised as expected. He was able to bear weight and move the ankle — cautiously, as one would — but without the level of incapacitation the injury had suggested was coming. This is consistent with what happens when the inflammatory terrain is addressed early: the cascade that would have entrenched the injury is interrupted before it has time to establish.
These accounts are anecdotal. They are two data points among many. They do not constitute evidence of a mechanism, nor are they presented as such. They are the kind of observations that prompt further enquiry — and that sit, in our view, coherently alongside what the scientific literature increasingly suggests about the role of pathogens in injury persistence and the potential of electromagnetic interventions.
How PHOENIX SANCTUM™ Approaches This
PHOENIX SANCTUM™ does not diagnose infections. It does not claim to treat disease. What it does is support the body's terrain — the informational, circulatory, and coherence conditions that allow the organism's own regulatory and immune processes to function more effectively.
When a client presents with chronic, unresolved pain at an injury site — particularly one that has not responded to conventional approaches — we consider the full terrain picture. This includes the possibility that microbial activity may be contributing to the persistence of inflammation. We use biofeedback scanning as an informational tool to identify resonance patterns of interest, not as a medical diagnostic instrument. We then build a frequency programme around the findings, layering antimicrobial resonance programmes with tissue-specific healing and circulatory support.
Technologies we may draw on for this kind of work include: cold laser applied locally, TENS silver bands or contact electrodes for direct electrical delivery at the site, PEMF for systemic and localised circulatory and cellular support, and — where the client is on a remote programme — continuous frequency delivery via sample-based remote support running in the background between sessions.
The aim is always the same: to help restore the conditions in which the body's own intelligence can complete what it started. Not to override nature, but to support the terrain so that nature can get in and do its work.
What You Can Explore
If you or someone you care about has been living with pain or inflammation at an old injury site that simply will not resolve — particularly if conventional approaches have delivered limited or temporary relief — this is worth considering.
We are not suggesting that every unresolved injury has a microbial component. The terrain is complex, and causes are rarely singular. But the science is clear that biofilm-mediated persistence is far more common than conventional medicine has historically acknowledged, and that the tools to address it extend beyond the pharmacological.
If you would like to explore how PHOENIX SANCTUM™ may be able to support your terrain — whether in person at our Dee Why clinic or via our structured remote pathway — we invite you to reach out at info@phoenixsanctum.com or visit www.phoenixsanctum.com to learn more about our service pathways.
References
[1] Costerton JW, Stewart PS, Greenberg EP (1999). Bacterial biofilms: a common cause of persistent infections.. Science 284(5418):1318–1322.
[2] Hall-Stoodley L, Costerton JW, Stoodley P (2004). Bacterial biofilms: from the natural environment to infectious diseases.. Nature Reviews Microbiology 2(2):95–108.
[3] Peel TN (2019). Studying Biofilm and Clinical Issues in Orthopedics.. Frontiers in Microbiology.
[4] Nishitani K et al. (2015). Quantifying the natural history of biofilm formation in vivo during the establishment of chronic implant-associated S. aureus osteomyelitis in mice.. Journal of Orthopaedic Research 33(9):1311–1319.
[5] Millar NL et al. (2020). A systematic review of inflammatory cells and markers in human tendinopathy.. BMC Musculoskeletal Disorders.
[6] Gracey E et al. (2020). Tendon and ligament mechanical loading in the pathogenesis of inflammatory arthritis.. Nature Reviews Rheumatology.
[7] Torp M et al. (2021). Effects of Resonant Electromagnetic Fields on Biofilm Formation in Pseudomonas aeruginosa.. Applied Sciences 11(16):7760.
[8] Shamis Y et al. (2025). Impact of high frequency electromagnetic radiation on bacterial survival and antibiotic activity in exposed bacteria.. Scientific Reports.
[9] Caubet R et al. (2004). A Radio Frequency Electric Current Enhances Antibiotic Efficacy against Bacterial Biofilms.. Antimicrobial Agents and Chemotherapy.
[10] Assaly R et al. (2022). Laser therapy versus pulsed electromagnetic field therapy for early knee osteoarthritis: a randomized controlled trial.. BMC Geriatrics.
[11] PEMF-Devices.com. Cold Laser Therapy / Low-Level Laser Therapy (LLLT) — Research Summary.. PEMF-Devices Research Database.